Shortly after the discovery of phages, scientists and physicians realised their therapeutic potential. Phage therapy is the direct administration of lytic phages to a patient with the purpose of killing the bacterial pathogen that is causing a clinically relevant infection - you can read more in our review article "Phage therapy in the post-antibiotic era". During the pre-antibiotic era, great interest arose around phage therapy. Then Alexander Fleming discovered penicillin in 1928 and the entire world changed.
Not even a century has passed since the discovery of antibiotics. However, it is difficult to imagine life without them. Antibiotic therapy has saved millions of lives and has been pivotal for medical breakthroughs such as organ transplantation and cancer chemotherapy. The possibility of losing antibiotic therapy as a resource in healthcare is truly frightening. But it is happening. Antibiotic resistance is a naturally-occurring event. Bacteria can be intrinsically resistant to one or more antibiotics, but can also acquire resistance traits through numerous genetic mechanisms. Furthermore, human activity -especially antibiotic overuse- greatly accelerates the processes driving antibiotic resistance. Add in the factor of a dry pipeline in antibiotic research and development, and we have the reasons behind the "post-antibiotic era" that we are already amid.
Image shows Jeremy Barr and lab alumni Fernando-Gordillo Altamirano collecting wastewater samples to isolate bacteriophages against antimicrobial-resistant pathogens. Taken from the documentary 'Last Chance to Save a Life'.
Given these circumstances, it is unsurprising that interest towards phage therapy has been rekindled. Throughout the world, great work has been done to establish the effectiveness and safety of phage therapy. We were part of the team involved in the first reported case study that used intravenous phage therapy to save the life of a critically-ill patient in the United States (known as the 'Tom Patterson' case, which you can read from Washington Post and Time Magazine, with the published paper here). The significance of this work was highlighted as it not only proved the usefulness of phage therapy as an alternative to antibiotics, but the potential use of phages and antibiotics combined.
Our lab's research and translation of Phage Therapy
Phage Therapy research at The Barr Lab broadly focuses on understanding the fundamental biology of bacteriophages that infect and lyse clinical antibiotic resistant pathogens. Before we can effectively apply phage therapy in clinic, we first must understand how these viruses function alongside their clinical bacterial hosts.
Research from our lab in this space uncovered a new clinical paradigm whereby certain phages can re-sensitise their bacterial hosts to the antibiotics they use to resist. We found that bacteria were killed by phages, but quickly developed phage resistance. However, by understanding the fundamental biology and phage receptors, these phage-resistant bacteria were re-sensitised to certain antibiotics. We then conducted in vivo experiments utilising this "one-two punch" strategy to demonstrate the clinical utility of our approach.
We have established the Monash Phage Foundry (MPF) which serves as an in-house phage production facility to generate clinical-grade phage products for the treatment of local patients. The MPF has been designed to reliably produce phage products at scale that are safe for clinical administration.
We have also developed 'Phage Cocktails' against leading nosocomial pathogens that are highly drug-resistant. We developed an 'institution-specific' phage cocktail against an emerging clinical pathogen from a local hospital that had few treatment options available. We were able to produce this cocktail to a clinical-grade that enables us to administer our phage products to local patients enrolled through the VICPhage Service.
Image shows members of The Barr Lab in the Monash Phage Foundry (MPF) facility housed at Monash University, which provides clinical-grade production of bacteriophage products.
Gut Prophages
The human body contains an estimated thirty trillion microbial cells, with the large intestine harboring the most densely populated microbial ecosystem with 1013-1014 estimated microbial cells per gram of faecal matter. It is well established that our gut microbial flora is largely responsible for our overall health. Gut microbes have coevolved symbiotic relationships with our bodies, imparting specific functions associated with metabolism, maintenance of structural integrity of the gut mucosal barrier, immunomodulation, and protection against pathogens. Conversely, a faulty or dysbiotic gut microbiome can contribute to a range of gut disorders such as inflammation, metabolic diseases, cancers, and even impacting mental health. Hence, several studies have been conducted to define a "healthy human gut microbiome ".
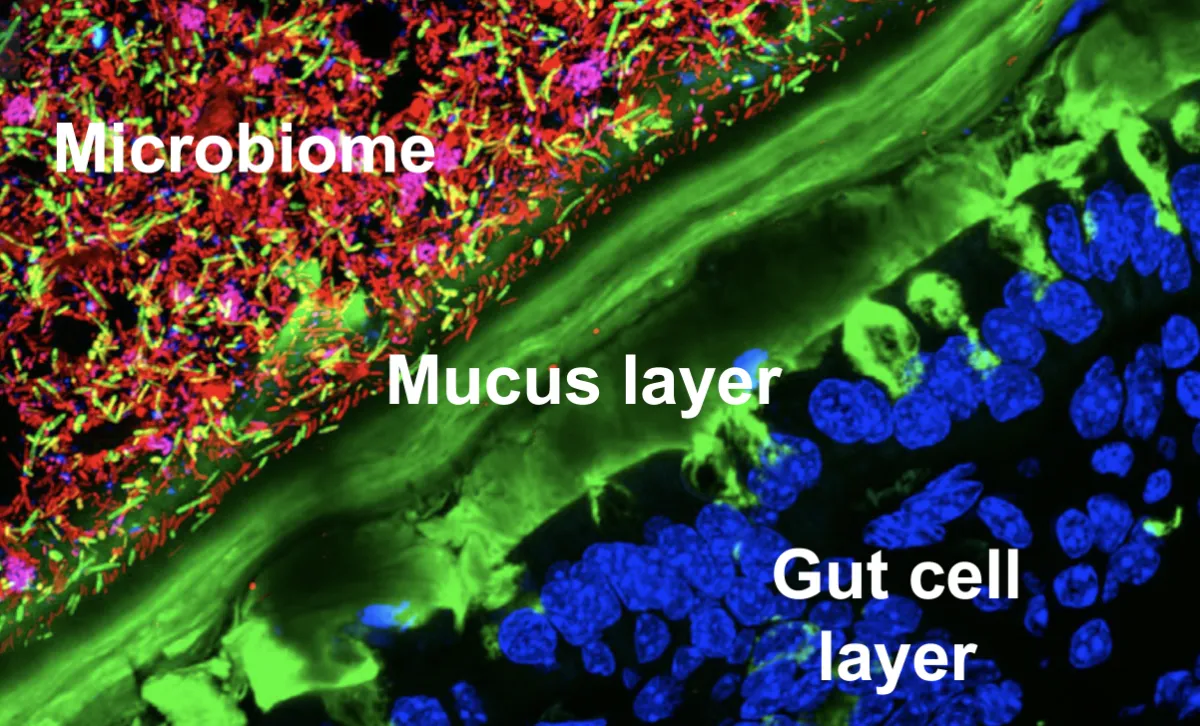
Image shows fluorescence microscopy cross-section of the gut epithelial cell layer with human gastrointestinal cell's nuclei stained blue, the mucosal surface lining the gut strained green, and the complex microbiome living inside us all stained red, pink, green, and blue.
Accordingly, the idea of a "healthy gut virome" has arisen. But identifying what a healthy virome is and how we can manipulate it, has remained largely out of reach. This is because our gut is complex and difficult to access, making its study challenging. As a result, most approaches utilize metagenomic sequencing in attempts to decipher the function of these gut bacteriophages.
The multitude of ways that bacteriophages influence their microbial hosts is becoming evident. Within the human gut, temperate appears to be the preferred phage lifecycle. Temperate phages integrate their genome within a host bacterium's genome as a prophage. Although temperate phages are not actively replicating in this lifecycle, the prophage is propagated and spread to daughter cells every time its bacterial host replicates. Prophages can encode a vast genomic repertoire which can provide novel functions, infer genomic plasticity, and increase the survival of their bacterial hosts. Prophages can be induced out of the temperate lifecycle back into the lytic lifecycle, lysing their bacterial host and releasing infectious phages back into the surrounding environment.
Our lab's research on the gut virome
The overwhelming majority of phages within our gut remain unidentified and unknown; only the tiniest scratch within a scratch on the surface has been made. At the Barr Lab, we are interested in identifying and characterising these gut prophages. However, our approach to do this, differs from the current status quo.
Through our collaborators, we have access to the Australian Microbiome Culture Collection, which contains thousands of human gut bacterial isolates. These isolates are whole-genome sequenced, stored in frozen samples, and can be cultured under anaerobic conditions. Using this resource, our work is just beginning to uncover the incredible function and biology of gut phages. We are now able to grow gut bacteria and their phages within anaerobic incubators within our labs, we have identified their genomes, can predict gut phage activity and function, and we are now beginning to produce these phages and apply them to complex gut microbial communities.
While this research is very early stage, this work has the potential to uncover never-before-seen biology of these understudied viruses and may even develop the tools and biological products (i.e., phages) that can be used to manipulate and control the human gut and its function.
Image shows anaerobic chamber at The Barr Lab, which allows us to culture gut bacteria and their prophages under anaerobic conditions. The entire chamber is kept at 37 °C and pumped with a complex mixture of CO2, Hydrogen, and N2 gases.
Phage-Mammalian
The human body is colonized by a diverse collective of microorganisms, including bacteria, fungi, protozoa and viruses. The smallest entity of this microbial conglomerate are the bacteriophages. Phages colonies all niches of the body, including the skin, oral cavity, lungs, gut and urinary tract. As such our bodies are frequently and continuously exposed to high numbers of phages, and we secrete more than several billion phages per gram of feces.
Phages cannot infect human cells in the same way they infect their bacterial host cells. Nevertheless, phages freely and profusely penetrate our bodies; having been found within the blood, serum, lung, liver, kidney and even within the brain. How phages are capable of crossing confluent epithelial cell barriers and accessing these 'classically sterile' regions of the body remained poorly understood.
Our lab's research on the phage-mammalian interactions
Research from The Barr Lab proposed some of the first mechanistic description on how bacteriophages can transcytosis (i.e., 'cross') cell layers. This process provides a generalized mechanism for phages to access the entire human body, whereby naturally occurring phages are endocytosed and transported across epithelial cell layers. In vitro studies demonstrated the rapid, directional transport of diverse phages across cell lines originating from across the body. Cell biology experiments revealed that phage particles could access all endo-membrane components of the mammalian cell, with phage transit occurring through the Golgi apparatus before being functionally exocytosed on the contralateral cell membrane.
Based on these results we estimate that the average adult human body transcytoses approximately 31 billion phages from the gut into the body every day. Naturally occurring phages can cross the confluent epithelial cell layers of the gut, gaining access to the body and result in the accumulation and assembly of an 'intra-body phageome'.
While it is now accepted that phages can rapidly enter human cells and organs through these processes, broader questions still remain. Chiefly, what are phages doing inside our own cells and bodies? While there are likely many answers to this question, our lab has been leading the field to decipher the cellular mechanisms that phages use to enter and traffic through our cell layers and have discovered that our cells do sense and respond to these intra-cellular viral wanderers.
Work from The Barr Lab has shown for the first time that one response to these intra-cellular viruses is for human cells to eat them. Using an array of techniques, including cell culture, immunology, and microarrays, we uncovered that human cells were engulfing bacteriophages and digesting them to increase their own cellular growth and proliferation. These findings are all done under experimental in vitro conditions, but suggest a diverse array of human responses and interactions to the bacteriophages that inhabit our bodies.
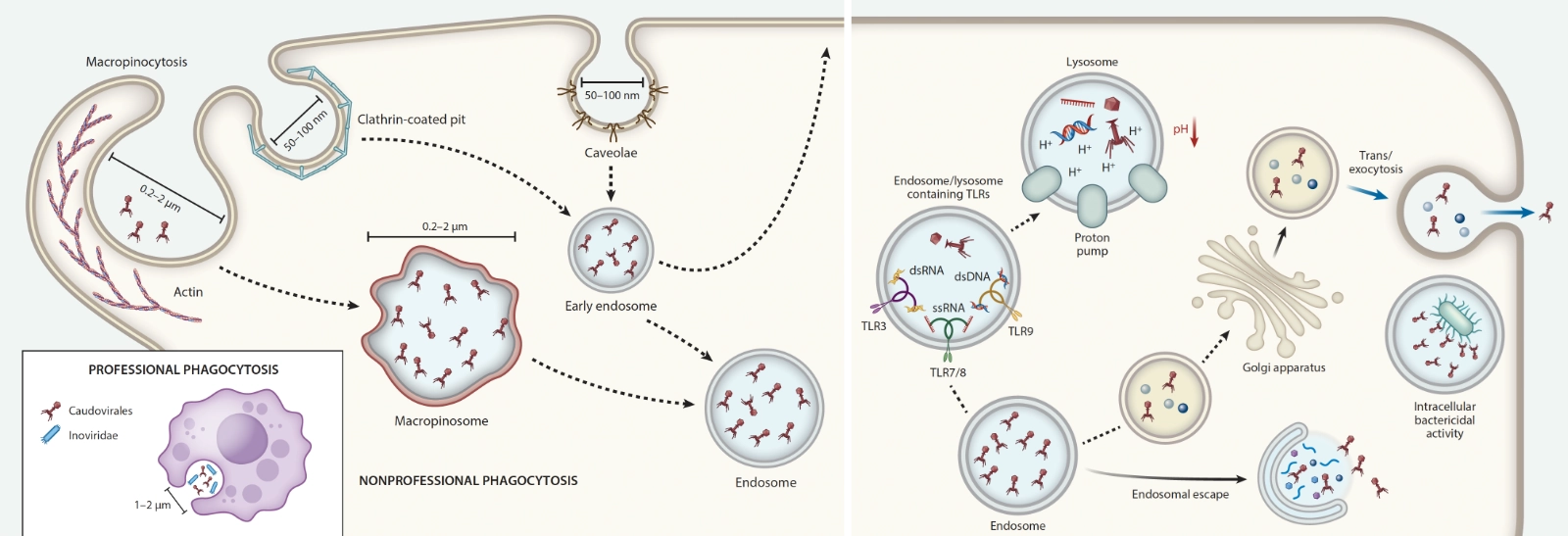
Image shows a schematic of a human cell internalising bacteriophages through macropinocytosis process. Phages are then trafficked throughout the cell structure in endomembrane-bound vesicles, where they can impart diverse functions and influences on the cell.